Disclaimer: The following guide is my best guess on what content will be on the exam. I do not know what exactly will be on the exam but I have helped over a thousand health care professionals pass the exam.
This content is protected by Canadian Copyright Laws. Your license number is embedded into the code of this web page and your computer IP address is tracked. Please do not reproduce. You are free to print out the highlighted guidelines and make notes. Thank you kindly.
Hypoglycemia in Adults- 2023 update
Importance: Very high- Re-read a few times, be very familiar with chapter
Approximate time recommended: 75 minutes
 Loading...
Loading...
Most of the content here is covered in the original chapter 14. The most important updates are the definition of hypoglycemia, the dosing of intranasal glucagon (Baqsimi), and reviewing the evidence on hypoglycemia with the newer insulins (which will become out of date again once insulin Icodec (the once weekly insulin) comes out in fall of 2024).
Under the heading of: Definition and Frequency of Hypoglycemia
Remember that the class of hypoglycemia is not defined by the blood glucose level but by symptoms and if the patient can help themselves or not. Know Table 1.
Please see the original chapter 14 for a review of the autonomic and neuroglycopenic symptoms start
Memorize Table 2
Know that effects the hypoglycemia can cause on the cardiovascular system, fall risk, a person’s quality of life, and the fear hypoglycemia can cause.
There are now scales that you can use to measure a person’s fear of hypoglycemia. Please see below.
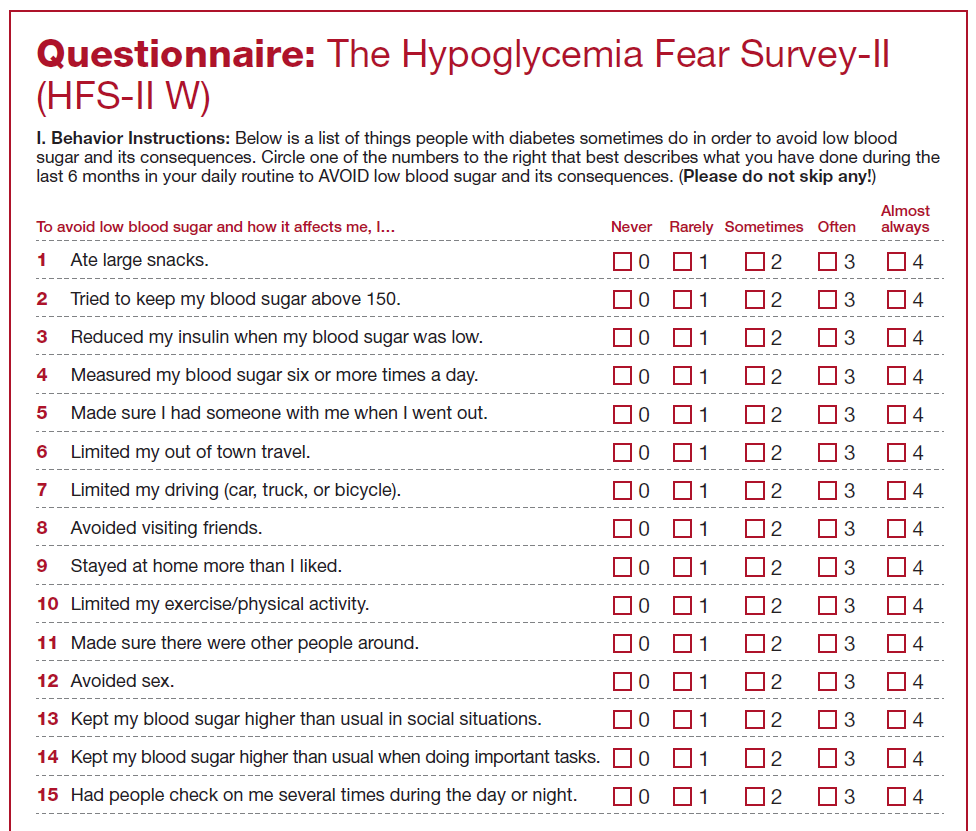
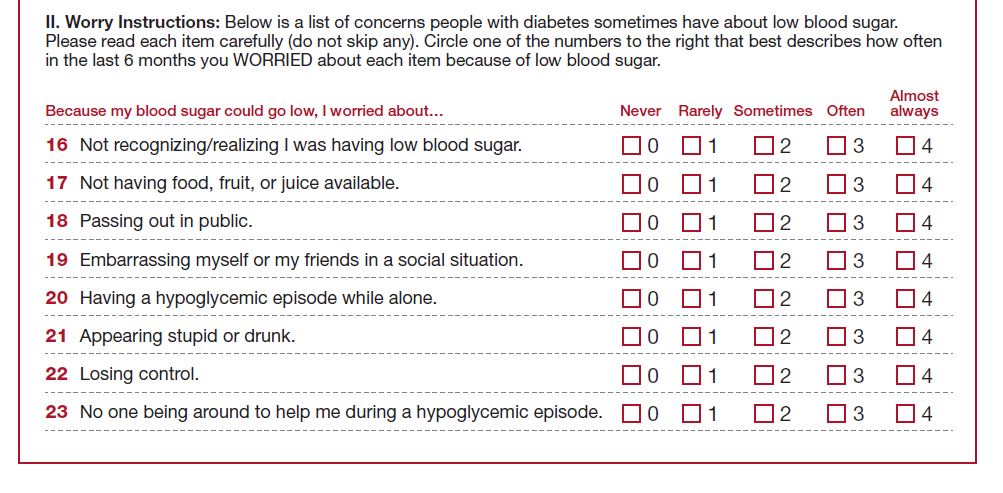
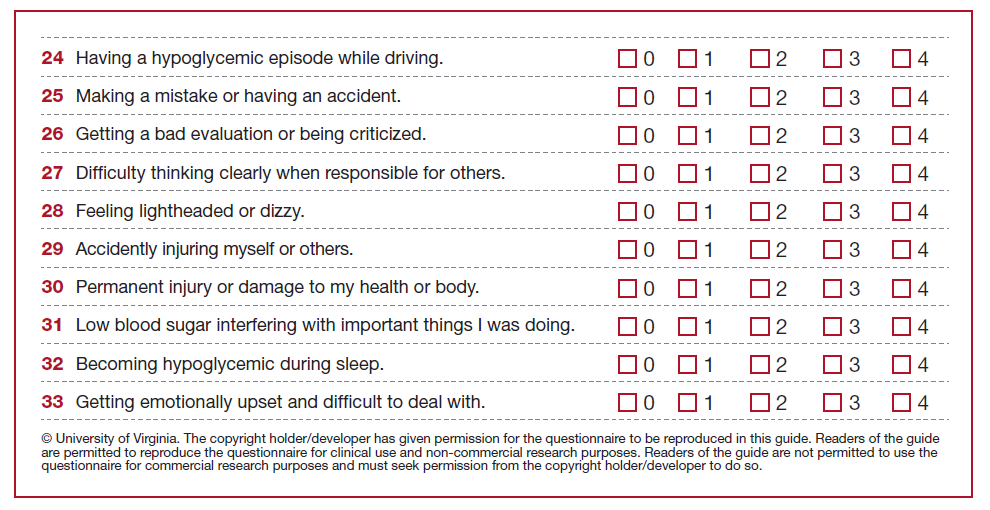
For more details on the The Hypoglycemia Fear Scale version 2 (HFS-II) please: see https://professional.diabetes.org/sites/default/files/media/ada_mental_health_workbook_chapter_4.pdf
Under the heading of: Prevention
Know which insulins and oral anti-hyperglycemics that have a lower risk of hypoglycemia
Know that structured psychoeducation programs such as HypoCOMPaSS (https://diabetesjournals.org/care/article/37/8/2114/29774/Recovery-of-Hypoglycemia-Awareness-in-Long) can reduce the prevalence of hypoglycemia
Know the interventions to prevent exercise induced hypoglycemia.
Under the heading of: Treatment
Know the amounts of carbohydrates, the does of IM/SC glucagon, and the dose of IN glucagon used to treat hypoglycemia. Memorize Table 4. Know what can interfere with glucagon.
This is not mentioned in the guidelines but pseudo-hypoglycemia is another form of hypoglycemia that patients can experience. This happens when a patient’s sugars have been high for a long time and the body adapts to this. The body thinks its “normal” for the sugars to be high. Then when you come along and bring the sugars to target the body thinks its “low” since its used to the high sugars as “normal”. Patients can experience symptoms of hypoglycemia even at sugars above 4 mmol/L. This is real and not just in the patient’s head. The treatment for this is to ease off on the medications so the body has time to adapt to the new lower sugars (usually this means titrating their insulin slower or even reducing the insulin dosage if the pseudo-hypoglycemia is happening often). Eventually the body will adjust to the new “low” sugars as “normal”. In my experience this takes a week or two. Treat pseudo-hypoglycemia as real hypoglycemia using fast acting carbohydrate but you could use a lower amount 5-10 grams. The symptoms your patient is experiencing are real and uncomfortable. So treat it as seriously as a real episode of hypoglycemia.
Frequently Asked Question- Why does alcohol stop glucagon from working?
When a person has hypoglycemia, glucagon secretion is stimulated from the alpha cells in a functional pancreas. Glucagon travels to the liver and stimulates the liver to convert its glycogen stores into glucose to raise blood sugars and treat the hypoglycemia. When alcohol is present, the liver is too busy processing the alcohol to respond to glucagon’s signal to convert glycogen to glucose. More specifically alcohol depletes nicotinamide adenine dinucleotide (NADH) which is required to break down glycogen into glucose. Without this enzyme glucagon doesn’t work and sugars do not increase. For more details into the biochemistry please see- http://pubs.sciepub.com/
You can order samples of Dex-4 from the manufacturer once you are a CDE. Where you work can be considered a diabetes clinic since you have your CDE. Please click on https://www.dex4.ca/diabetes-educators-join-us/
Practice Questions
Which of the following is true about the pathophysiology of hypoglycemia?
A) Myelinated nerves can readily break down glycogen into glucose to supply their energy needs
B) Neurons and glia rely on a constant supply of glucose. These cells are dependent on the bloodstream for this energy
C) A lack of glucose will likely cause a state of euphoric and blissful delirium
D) The sympathoadrenal response to hypoglycemia is increased due to sleep due to the dawn phenomenon
Which of the following insulins is associated with the lowest risk of hypoglycemia?
A) NPH
B) Tresiba (degludec)
C) Lantus (glargine-100)
D) Levemir (determir)